5 Surprising Realities of America’s Shift to Schedule III
For over half a century, federal policy maintained a “war on drugs” posture that treated cannabis as a “vicious external threat.” Since 1970, it sat in the most restrictive category possible—Schedule I—grouped with heroin and described as a substance with no medical value and a high potential for abuse. That era officially fractured on December 18, 2025, when President Donald Trump signed Executive Order 14370. This order directed federal agencies to move cannabis to Schedule III, reclassifying it alongside substances like ketamine, anabolic steroids, and Tylenol with codeine.
While the pivot recognizes the “accepted medical use” of the plant, the transition is a minefield of scientific paradoxes, regulatory traps, and lingering legal “gray areas.” As the administrative gears turn toward 2026, here are five surprising realities of America’s move to Schedule III.
1. Rescheduling is NOT Legalization (The “Safe Harbor” Paradox)
One of the most pervasive misconceptions is that rescheduling equates to federal legalization or decriminalization. It does not. Under Schedule III, cannabis remains a controlled substance, and federal criminal penalties for simple possession and trafficking stay on the books. While it acknowledges medical utility, it does not create a “get out of jail free” card for those operating outside strict federal pharmacy frameworks.
This creates a particular tension for veterans. Since April 2023, the Veterans Medical Marijuana Safe Harbor Act has been under consideration in Congress as a legislative attempt to bridge this divide. Without it, veterans remain in a “Safe Harbor” paradox: they are encouraged to discuss cannabis with their doctors under VHA Directive 1315, yet those same providers cannot prescribe it. For federal employees, the shift offers no protection; agencies maintain the authority to drug test and terminate employees for use.
“You might be illegal but we’re going to enact this law saying it’s legal even despite this other rule saying it’s illegal—it’s a safe harbor… Notably, if you’re a VA employee, you still can’t smoke weed.” — Casey Walker, Attorney and Founder of VA Disability Group

2. The “Gateway Drug” Theory is Scientifically Faltering
For decades, the “gateway drug” narrative was a cornerstone of U.S. policy. Emerging from a 1950s “top-to-bottom push” described by historians as an effort to portray cannabis as an external threat luring “innocent White youths,” the theory suggested cannabis use inevitably led to heroin and ruin.
Modern data has demolished this causality. Technical literature from 2024 and 2025 shows that cannabis initiation occurring before the use of tobacco or alcohol is remarkably rare, involving only 6% of users.
As the National Academies of Sciences, Engineering, and Medicine (NASEM) notes, sequencing does not imply causality. This realization marks a massive departure from a narrative once used to justify the systemic marginalization of “racialized minorities” under the guise of public health.
3. The “Driving Paradox”—Frequent vs. Occasional Users
As states liberalize cannabis laws, traffic safety has become a central concern. However, reports from the AAA Foundation for Traffic Safety reveal a counter-intuitive “driving paradox.” Researchers found that “lane departures” occur more often in occasional users than in daily users, who may learn to compensate for the drug’s effects or develop a physiological tolerance.
The real difficulty lies in roadside testing. Unlike the 0.08 BAC limit for alcohol, there is no scientific “per se” limit for THC. This is due to the highly lipophilic (fat-soluble) nature of cannabinoids. THC is stored in adipose tissue and redistributed back into the bloodstream for weeks after consumption, meaning a positive blood test does not necessarily prove acute impairment.
“The joint contribution of cannabis and alcohol to crash risk was not significantly larger than that caused by alcohol alone… There is a lack of a clear ‘per se’ limit for THC concentration, like the 0.08 BAC for alcohol.” — AAA Foundation Technical Report
4. Tax Relief vs. The “FDA Trap” for Businesses
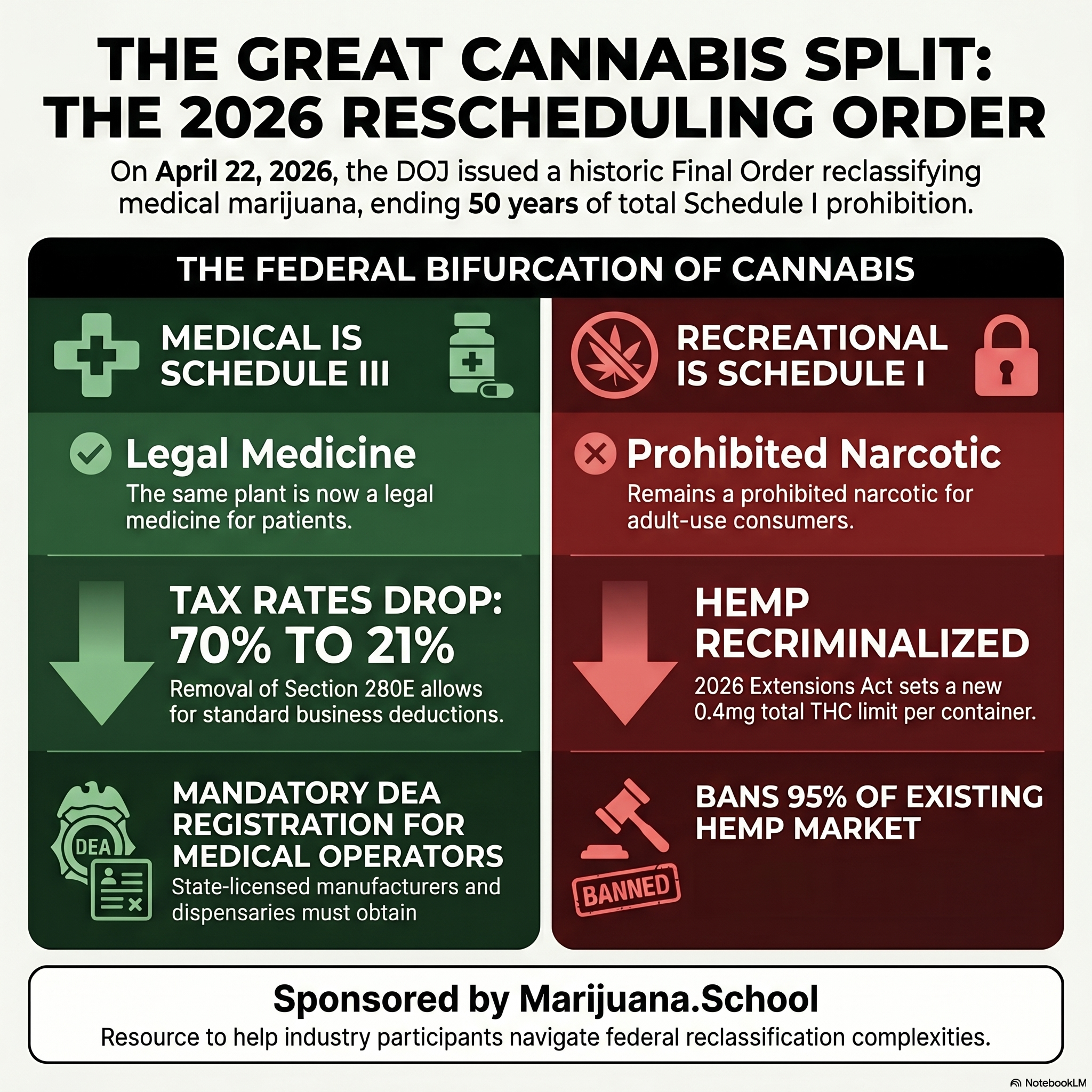
For the $32 billion cannabis industry, rescheduling offers a financial lifeline via the removal of Internal Revenue Code Section 280E. Currently, cannabis businesses are barred from deducting “ordinary and necessary” expenses like rent and payroll. Moving to Schedule III allows these deductions, though the impact is tiered: relief primarily benefits retailers, while manufacturers see more modest gains.
However, a “regulatory trap” looms. Schedule III brings cannabis into the FDA’s domain of pharmaceutical oversight. For small business owners like Ali Jamalian—the San Francisco-based CEO of Sunset Connect who describes his ubiquitous pre-roll brand as the “Bud Light of weed”—the costs of traditional FDA approval are impossible.
The Financial Pivot:
- The Win: Deductibility of rent, insurance, and payroll, potentially lowering effective tax rates that are currently up to four times higher than other industries.
- The “Dragonglass” Dilemma: Jamalian patented “Dragonglass,” a cannabis-derived formulation that helped manage his wife’s severe epilepsy. While rescheduling may invite pharmaceutical interest in licensing such patents, bringing a new drug to market costs an average of $1 billion and takes 12 years—a hurdle no current cannabis company can clear alone.
5. Medical Promise Meets Cardiovascular Reality
Federal acknowledgment of medical utility is a watershed moment, but the scientific community remains cautious. While some outcomes are well-documented, others remain in a “therapeutic gray area.” Notably, the reclassification applies only to the plant; synthetically derived cannabis remains under the restrictive Schedule I.
Medical Evidence: Proven vs. Speculative
- Conclusive/Substantial Evidence: Treatment of chronic pain in adults; chemotherapy-induced nausea; and rare pediatric epilepsy (FDA-approved Epidiolex).
- Limited/Inconsistent Evidence: Treatment of glaucoma, certain cancers, and symptoms of Tourette syndrome.
Furthermore, physicians warn of “biphasic effects,” where the drug’s impact reverses based on dosage. While low doses may reduce anxiety, high doses can trigger it. This same biphasic nature applies to Male Sexual Behavior (MSB): low doses can enhance desire and satisfaction, while high doses are linked to erectile dysfunction and inhibited orgasm. Perhaps most concerning is the emerging link between acute use and myocardial infarction (heart attacks) and strokes, even in young, healthy individuals.
The 2026 Horizon and a Ponderable Future
The rescheduling process is accelerating. While the DEA public hearing was originally delayed, it is now set for January 21, 2025. Attorney General Pam Bondi has been ordered to act “expeditiously,” a directive that legal experts believe could lead her to waive the public comment period entirely to finalize the rule.
With Robert F. Kennedy Jr. leading Health and Human Services and “drug czar” nominee Sara A. Carter overseeing policy alongside “psychedelics czar” Matthew Zorn, the administration seems poised to favor a research-heavy, pharmaceutical-friendly framework. Yet, a fundamental question remains: with nearly 70% of the public demanding full federal descheduling, will this “middle ground” survive the inevitable court challenges from groups like Smart Approaches to Marijuana?
Ponderable: Is the shift to Schedule III a genuine bridge to a new era of medical discovery, or a regulatory bottleneck designed to favor pharmaceutical giants over the craft neighborhood dispensaries that built the industry?